Recessed vs Normal Maxilla: Key Differences Explained
Learn the visual and structural differences between a recessed vs normal maxilla, how it affects facial appearance, and what options exist to address it.
The maxilla is one of the most consequential bones in the face, yet most people have never heard of it until they start paying close attention to facial structure. If you have ever looked in the mirror and felt like your midface looks flat, your under-eye area looks hollow, or your profile lacks forward projection, the maxilla is likely part of the equation.
Understanding the difference between a recessed and a normal maxilla gives you a clearer picture of what you are actually working with, and what, if anything, can be done about it.
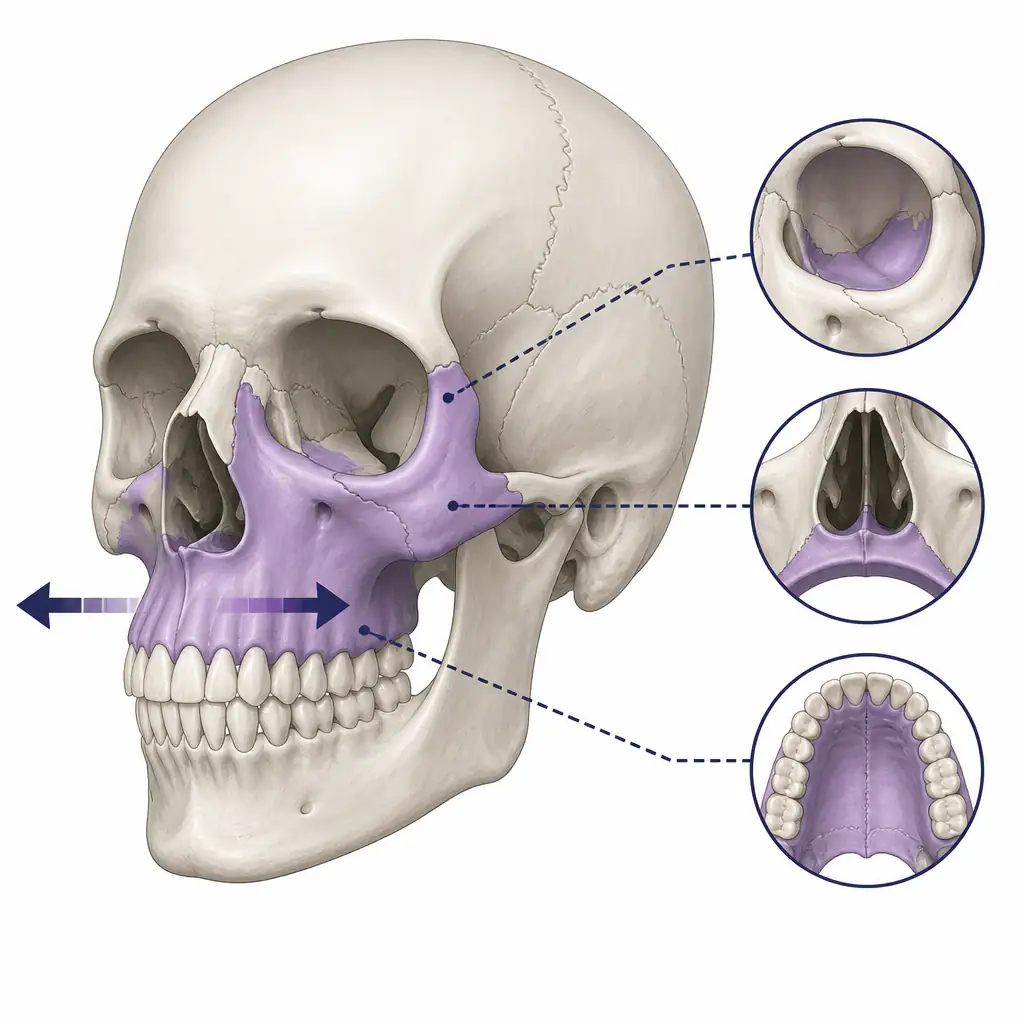
What Is the Maxilla?
The maxilla is a paired facial bone that forms the upper jaw, the floor of the eye sockets, the sides of the nasal cavity, and a significant portion of the hard palate. It is not just a tooth-holder. It is a structural foundation for the entire midface.
When the maxilla sits in its ideal position, it provides forward support to the cheeks, the under-eye area (the infraorbital region), and the base of the nose. It also positions the upper teeth correctly in relation to the lower jaw, which affects both bite function and facial aesthetics.
The position of the maxilla is described in three planes:
- Anteroposterior (AP): How far forward or backward it sits
- Vertical: How high or low it sits, affecting tooth display and lip posture
- Transverse: How wide it is, affecting palate width and nasal breathing
When people talk about a recessed maxilla, they are almost always referring to the anteroposterior plane, meaning the bone does not sit far enough forward.
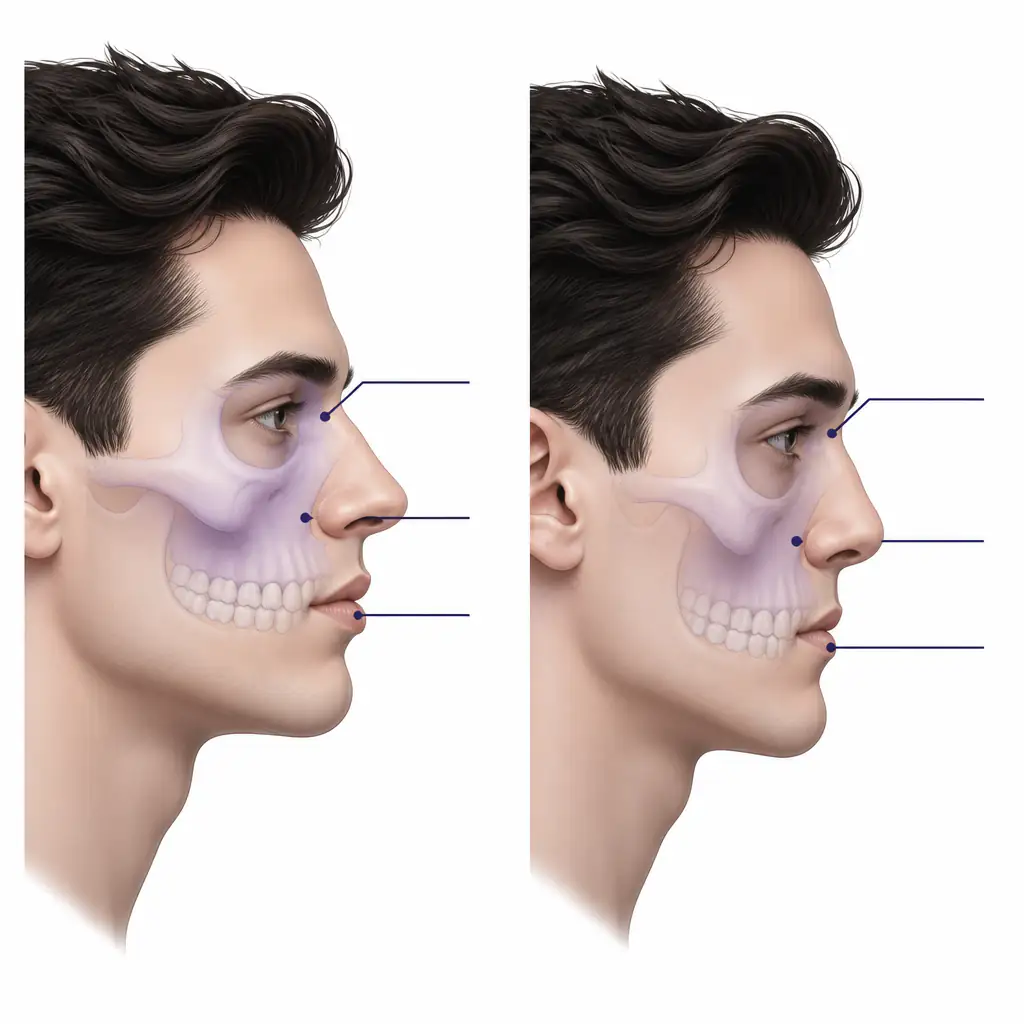
What Does a Normal Maxilla Look Like?
A normally projected maxilla creates several visual landmarks that most people associate with an attractive or balanced midface:
- Flat or slightly positive orbital vector: The cheekbone and infraorbital rim sit at or in front of the eyeball when viewed from the side
- Full under-eye support: Little to no hollow or “tear trough” appearance
- Forward cheek projection: The lateral midface has volume and appears lifted
- Adequate nasolabial angle: The base of the nose has proper support
- Upper lip support: The upper lip sits slightly forward, not tucked inward
In profile, a person with a well-projected maxilla will typically show a relatively straight or slightly convex facial line from the forehead down through the midface to the chin. The midface does not appear to “cave in” between the brow ridge and the mouth.
Orthognathic (jaw and facial bone) surgeons often use cephalometric landmarks to assess maxillary position precisely. One common reference is the Nasion-A point relationship, where point A (the deepest point of the curve above the upper incisors) is measured against a vertical line dropped from Nasion (the bridge of the nose). In a normally projected maxilla, point A sits at or near that vertical line.
What Is a Recessed Maxilla?
A recessed maxilla, sometimes called a hypoplastic maxilla or maxillary retrusion, means the bone sits further back than its ideal position. The degree of recession can range from subtle to severe.
Common visual signs of a recessed maxilla include:
- Negative orbital vector: The eye appears to protrude forward relative to the cheekbone and infraorbital rim
- Under-eye hollowing or dark circles caused by lack of bony support beneath the orbital rim
- Flat or “sunken” midface appearance
- Prominent nasolabial folds appearing earlier or more deeply
- Upper lip that appears thin or tucked in due to lack of anterior support
- Retruded upper teeth or a tendency toward an underbite, depending on lower jaw position
- Class III malocclusion in more pronounced cases, where the lower teeth sit in front of the upper teeth
It is worth noting that a recessed maxilla does not always mean poor facial aesthetics. Facial appearance is the product of multiple structures working together, and a person with a slightly recessed maxilla but strong cheekbones, good soft tissue, or a well-positioned lower jaw may still have an attractive face overall.
Recessed vs Normal Maxilla: Side-by-Side Comparison
Here is a direct comparison across the key features that distinguish these two presentations:
| Feature | Normal Maxilla | Recessed Maxilla |
|---|---|---|
| Orbital vector | Flat or positive (cheek at/forward of eye) | Negative (eye protrudes past cheek) |
| Under-eye area | Supported, minimal hollow | Hollow, “tear trough” appearance |
| Cheek projection | Forward and defined | Flat or absent |
| Upper lip posture | Naturally full, forward | Thin, tucked, or retruded |
| Profile line | Straight or convex midface | Concave midface (“dished” appearance) |
| Nasolabial folds | Shallow or absent in youth | More prominent, earlier onset |
| Bite tendency | Class I (neutral) | Risk of Class III or compensated bite |
| Nasal base support | Adequate, stable | Can appear pinched or drooping |
This is a general guide. Individual variation is significant, and a qualified orthodontist or maxillofacial surgeon is the only professional who can accurately assess your actual maxillary position using imaging.
What Causes Maxillary Retrusion?
Maxillary position is primarily determined by genetics, but several factors can influence development:
Genetic Factors
Familial patterns of maxillary retrusion are common. Certain ethnic populations also have different baseline maxillary norms, which is why cephalometric standards have historically varied across populations.
Mouth Breathing During Development
Research suggests that chronic mouth breathing in childhood may alter craniofacial development. When the tongue does not rest on the palate (its natural resting position), the transverse and vertical development of the maxilla can be affected. This is one reason mewing (maintaining proper tongue posture) has attracted interest, though evidence for its effects in adults remains limited.
Premature Tooth Loss or Orthodontic History
Extraction-based orthodontics, once common, involved removing premolars to create space for crowding. Some researchers argue this can reduce forward development of the dental arches, though this remains debated in the literature.
Midface Trauma or Cleft-Related Conditions
Trauma to the midface during development, or conditions like cleft palate, can directly alter maxillary growth trajectory.
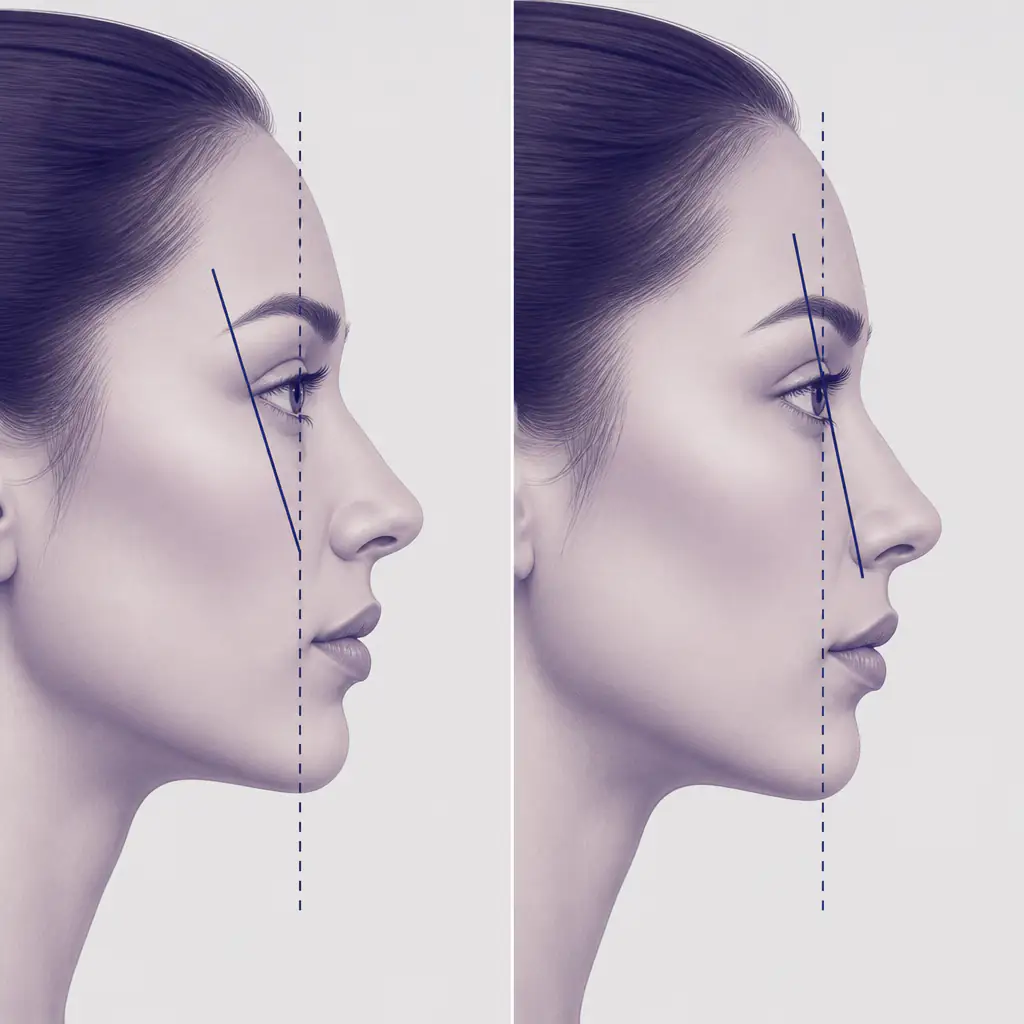
How to Assess Your Own Maxillary Position
You do not need a clinical setting to get a rough sense of your maxillary projection. There are a few practical self-checks:
1. The orbital vector check Look at a side-profile photo. Draw a mental line from your cheekbone (malar eminence) straight down. If your eye appears to sit behind that line, your orbital vector is positive. If your eye appears to sit in front of that line, your vector is negative, which often corresponds with maxillary retrusion.
2. The finger test Place your finger flat against your cheekbone and tilt it slightly toward your eye. If your lower eyelid and the area beneath it sink noticeably behind your finger, you likely have a negative orbital vector.
3. Profile photo analysis Take a neutral side profile photo. Look at the midface line from your brow ridge to your upper lip. A straight or slightly forward-curving line suggests normal projection. A curved-inward or “concave” midface line often indicates retrusion.
For a more structured baseline assessment, tools like Aura can analyze facial structure from photos, including orbital vector and midface projection, giving you a data-driven starting point before you decide whether to pursue any intervention.
What Can Be Done About a Recessed Maxilla?
Options vary widely depending on the degree of retrusion and whether skeletal growth is still occurring.
Non-Surgical Approaches
Tongue posture and mewing: Maintaining proper tongue posture (tongue flat on the roof of the mouth, lips together, teeth lightly touching) is theorized to support natural maxillary development. In growing individuals, some practitioners believe this may support forward growth. In fully developed adults, effects are more limited and not well-documented in controlled studies.
Palate expanders: Orthodontic expanders widen the transverse dimension of the maxilla. In children and adolescents, this is well-supported. Devices like the MARPE (Miniscrew-Assisted Rapid Palate Expander) have shown some success in young adults as well, though results vary.
Orthodontic compensation: In cases of mild discrepancy, orthodontics can adjust tooth positions to create a functional bite and improved appearance without moving the bone itself.
Surgical Approaches
Le Fort I osteotomy: This is the primary surgical procedure for correcting maxillary retrusion. The maxilla is surgically repositioned forward (advanced) and fixed in the new position. It is a significant procedure performed by oral and maxillofacial surgeons, typically in combination with treatment of the lower jaw (bimaxillary surgery) when needed.
Distraction osteogenesis: Used in more severe cases, this technique gradually moves bone forward over weeks using a distraction device.
Facial implants: Infraorbital and malar (cheekbone) implants do not move the bone but can restore volume and projection to areas made deficient by a recessed maxilla. They are less invasive than osteotomy but address appearance rather than skeletal position or bite.
If you are considering any surgical procedure, consult with a board-certified oral and maxillofacial surgeon or craniofacial specialist. These are complex interventions with real risks, and only a qualified professional can evaluate whether you are a candidate.
Practical Takeaways
If you are trying to understand where your own facial structure falls:
- Assess objectively first. Use photos taken from neutral angles in good lighting. Avoid making judgments based on unflattering or distorted images.
- Consider the full picture. Maxillary projection interacts with lower jaw position, cheekbone size, soft tissue thickness, and many other variables. One feature does not define an entire face.
- Track changes over time. If you are pursuing any lifestyle or orthodontic approach, consistent photo documentation helps you evaluate whether anything is actually changing.
- Get professional input before acting. For anything beyond posture or lifestyle changes, a consultation with an orthodontist, oral surgeon, or facial plastic surgeon is the appropriate step.
Using Aura to get a scored breakdown of your facial structure, including midface and under-eye analysis, can help you identify which areas are actually affecting your overall aesthetic before investing time or money in any specific intervention.
Frequently asked questions
Can you fix a recessed maxilla without surgery? +
Non-surgical options are limited in fully grown adults. Tongue posture practices and palate expanders may have some effect in younger individuals or adolescents, but for significant maxillary retrusion in adults, surgical options like Le Fort I osteotomy are the most reliable correction. Consult a qualified maxillofacial surgeon to understand what applies to your specific situation.
How do I know if I have a recessed maxilla? +
Common signs include a negative orbital vector (eye appears to protrude past the cheekbone in profile), hollowing under the eyes, a flat or concave midface profile, and an upper lip that appears tucked or thin. A definitive assessment requires cephalometric X-ray analysis by an orthodontist or oral surgeon.
Does a recessed maxilla affect breathing or dental health? +
Yes, it can. A narrow or recessed maxilla may contribute to nasal airway restriction, sleep-disordered breathing, and malocclusion (poor bite alignment). In some cases, palate expansion or surgical correction improves both function and appearance simultaneously.
Is maxillary retrusion the same as an underbite? +
Not exactly. An underbite (Class III malocclusion) can result from a recessed maxilla, but it can also come from an overdeveloped lower jaw, or a combination of both. The distinction matters because the treatment approach differs depending on which structure is contributing to the discrepancy.