Mandible vs Maxilla: Key Differences Explained
Learn the key differences between the mandible vs maxilla, how each bone shapes your face, and what you can do to optimize both for better facial harmony.
Your face is built on a scaffold of bone, and two structures sit at the center of that scaffold: the mandible and the maxilla. Most people have heard of the jawline, but fewer understand the distinct roles these two bones play in determining how a face looks at rest, in motion, and from every angle.
This article breaks down exactly what each bone does, how they differ structurally and functionally, and why the relationship between them matters more than either bone in isolation.
What Is the Mandible?
The mandible is the lower jaw. It is the only freely movable bone in the human skull, articulating with the temporal bone on each side via the temporomandibular joint (TMJ). Every time you speak, chew, or yawn, the mandible is doing the work.
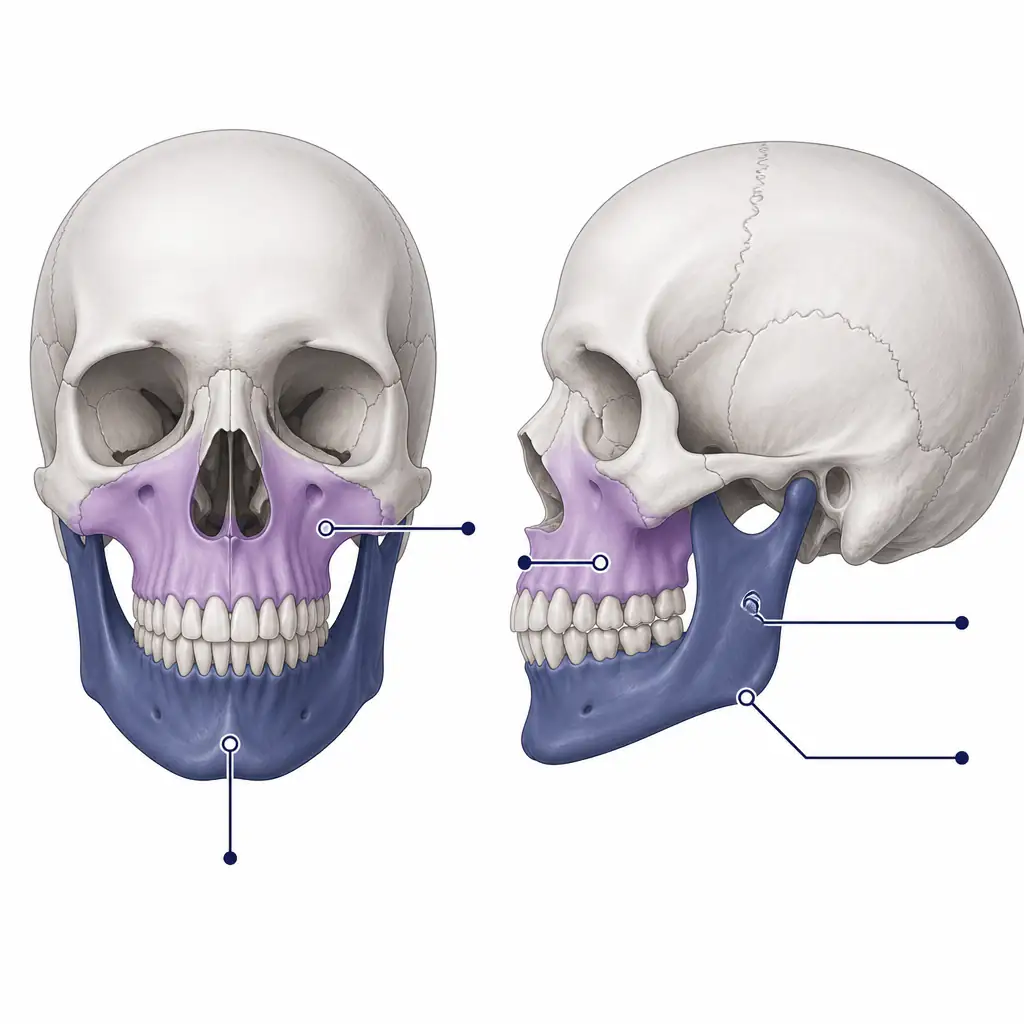
From an aesthetic standpoint, the mandible defines the lower third of the face. Its key landmarks include:
- The body: the horizontal portion that holds the lower teeth
- The ramus: the vertical portion on each side that rises toward the ear
- The gonial angle: the corner where the body meets the ramus, sometimes called the jaw angle
- The chin (mental symphysis): the midpoint projection at the front
- Condyles: the rounded ends that fit into the skull to form the TMJ
A well-developed mandible typically features a defined gonial angle, strong chin projection, and sufficient width across the lower face. These traits are consistently rated as attractive in peer-reviewed research on facial aesthetics.
What Is the Maxilla?
The maxilla is the upper jaw. Unlike the mandible, it is fixed, meaning it does not move on its own. It is actually a paired bone, with a left and right half that fuse at the midline during development. The maxilla sits at the center of the mid-face and connects to nearly every other facial bone, including the zygomatic (cheekbones), nasal bones, and the floor of the eye sockets.
The maxilla’s key anatomical roles include:
- Supporting the upper teeth and hard palate
- Forming the floor and walls of the nasal cavity
- Contributing to the orbital floor (the base of the eye socket)
- Providing the structural platform for the cheeks and midface
Aesthetically, maxillary development is closely tied to midface projection, cheekbone prominence, and the appearance of the nose. A well-projected maxilla tends to push the midface forward, giving the face a more three-dimensional, forward-grown look. A retracted or underdeveloped maxilla can create a “sunken” midface appearance, affect nasal support, and influence how the lips sit at rest.
Mandible vs Maxilla: Side-by-Side Comparison
| Feature | Mandible | Maxilla |
|---|---|---|
| Location | Lower jaw | Upper jaw / midface |
| Mobility | Freely movable | Fixed (fused to skull) |
| Bone count | Single bone | Paired bones (fused) |
| Teeth supported | Lower 16 teeth | Upper 16 teeth |
| Key joint | Temporomandibular joint (TMJ) | None (sutural connections) |
| Aesthetic influence | Chin, jaw width, jaw angle | Midface projection, cheeks, eye area |
| Articulates with | Temporal bone (skull) | Cheekbones, nasal bones, orbital floor, palatine bones |
| Growth completion | Late teens to early 20s | Mid teens, slightly earlier |
The core difference is structural role. The mandible is a moving frame, defining the lower face’s shape and driving jaw function. The maxilla is a fixed platform, anchoring the midface and providing the foundation that everything above and below it relates to.
How Each Bone Affects Facial Aesthetics
Mandible and Facial Aesthetics
The mandible’s contribution to attractiveness is heavily discussed in facial assessment. Three traits tend to matter most:
- Chin projection: How far the chin protrudes relative to the rest of the face. Measured using the Frankfort horizontal plane, a well-projected chin aligns roughly with or slightly behind a vertical line dropped from the most forward point of the upper lip.
- Bigonial width: The distance between the two gonial angles. A wider bigonial measurement generally produces a more defined, squared jaw silhouette.
- Gonial angle: Acute gonial angles (roughly 115 to 125 degrees) are often associated with a sharper, more angular jaw appearance. Very obtuse angles tend to produce a rounded, less defined jaw.
Maxilla and Facial Aesthetics
Maxillary development has a cascading effect on the whole face. Because the maxilla connects to so many adjacent structures, its size and projection influence:
- Orbital support: The maxilla forms part of the orbital rim, so underdevelopment can contribute to under-eye hollowing or a tired appearance.
- Nasal support: The nasal base rests partly on the maxilla. Insufficient forward projection can lead to a drooping nasal tip.
- Lip posture: Lip fullness and positioning at rest partly depends on the underlying maxillary bone. A forward-positioned maxilla supports fuller-looking lips.
- Cheek projection: The zygomatic process of the maxilla blends into the cheekbones, so strong maxillary growth contributes to prominent cheeks.
In facial assessment frameworks like those used in orthognathic surgery planning, the maxilla is often evaluated first, because its position sets the reference for evaluating the mandible’s relative position.
The Relationship Between the Two Bones
Thinking about the mandible and maxilla in isolation misses the bigger picture. What truly drives facial harmony is the relationship between the two bones, captured in part by the concept of occlusion (how the upper and lower teeth fit together) and sagittal jaw relationship.
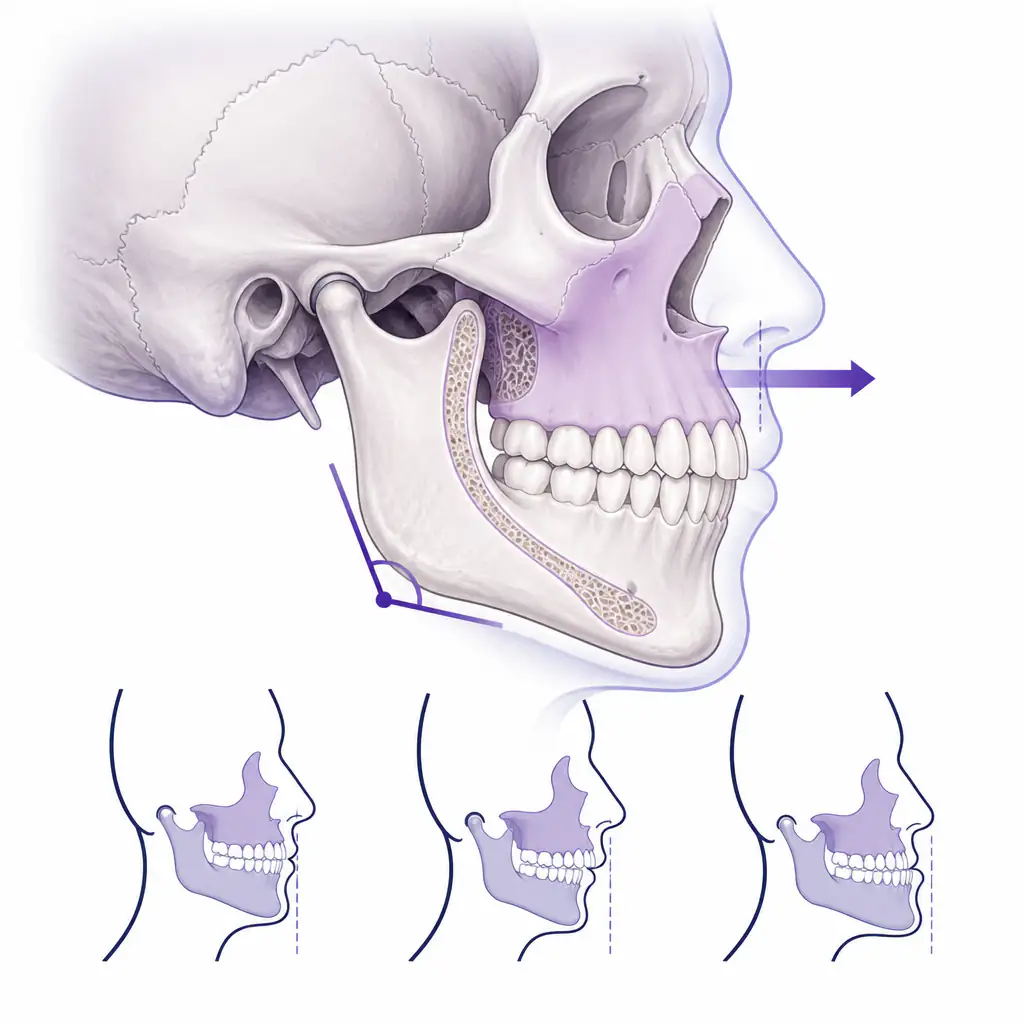
Orthodontists classify jaw relationships into three skeletal classes:
- Class I: The upper and lower jaws are in good relative position. Upper teeth sit slightly in front of lower teeth. Generally considered the standard reference.
- Class II: The mandible is relatively set back compared to the maxilla (or the maxilla protrudes forward). Often associated with a recessed chin and prominent overbite.
- Class III: The mandible protrudes relative to the maxilla. Associated with an underbite and a chin that appears to jut forward.
These classifications matter beyond dentistry. Skeletal class affects profile shape, how the nose and chin relate to each other, and overall facial balance. Many looksmaxxing discussions focus on only one bone, but correcting or optimizing one without considering the other can produce unbalanced results.
If you want a structured starting point for understanding how your own jaw proportions compare to established facial harmony benchmarks, Aura offers AI-powered jawline analysis and facial scoring that breaks down individual features rather than giving a single number.

Can These Bones Be Changed?
This is where the conversation becomes more nuanced. Bone is living tissue and, during periods of growth, is responsive to environmental forces. After growth plates close, changes to bone structure generally require either surgical intervention or indirect approaches.
During Growth
During adolescence, both the mandible and maxilla are still developing. Orthodontic and orthopedic interventions can have meaningful effects:
- Palatal expanders widen the maxilla by slowly separating the midpalatal suture, which remains unfused until early adulthood.
- Functional appliances (like the Herbst appliance or Twin Block) can influence mandibular growth direction in growing patients.
- Mewing (maintaining proper tongue posture against the hard palate) is often discussed in this context. Research on its skeletal effects is limited, but some practitioners suggest it may support proper maxillary development when practiced consistently during growth years.
After Growth
For adults with fully fused sutures, skeletal changes require surgical approaches:
- Orthognathic surgery involves moving the maxilla (Le Fort I osteotomy), mandible (BSSO), or both to correct skeletal discrepancies. It is a significant procedure with a real recovery period and genuine functional and aesthetic results.
- Genioplasty specifically addresses chin projection by repositioning or reshaping the chin bone.
- Implants (chin or jaw angle implants) can augment the apparent shape of the mandible without moving bone.
- MARPE (Miniscrew-Assisted Rapid Palatal Expansion) is a newer technique that can expand the maxillary suture in adults using skeletal anchorage.
Talk to a qualified oral and maxillofacial surgeon or orthodontist before considering any of these procedures. What works for one skeletal pattern may be inappropriate or counterproductive for another.
Practical Tips for Assessing Your Own Jaw Structure
You do not need a clinical setting to get a reasonable sense of your own mandible and maxilla development. Here are some practical self-assessment approaches:
- Take a lateral (side profile) photo. A true profile shot with neutral lighting tells you more about chin projection and midface depth than a front-facing photo.
- Check your lip posture at rest. Are your lips together comfortably without muscular strain? Lips that strain to close can suggest skeletal discrepancy.
- Look at your midface from a three-quarter angle. A flat midface from this angle often indicates limited maxillary projection.
- Assess your gonial angles. From a front-on photo, the jaw corners should be visible. If the lower face tapers sharply from cheekbones to chin with no visible jaw angle definition, bigonial width may be limited.
- Use an AI facial analysis tool for an objective baseline. Subjective self-assessment is prone to bias. Aura can score your jawline, chin projection, and overall facial structure against thousands of reference points, giving you a more grounded starting point before deciding what, if anything, to address.
Common Misconceptions
“The jaw is just the chin.” The mandible includes the full lower jaw structure. Chin work alone does not address jaw width or angle definition.
“Maxilla only affects the upper teeth.” The maxilla’s influence extends to the eye area, cheeks, nose, and lips. It is a central hub of the face.
“Mewing will reshape adult bone.” Current evidence does not support significant skeletal changes from tongue posture in fully grown adults. It may help with soft tissue positioning and muscle tone, but bone-level claims are overstated.
“Bigger is always better.” Facial aesthetics are relational. A large mandible relative to a small maxilla, or vice versa, tends to look less balanced than proportionate development of both.
Frequently asked questions
What is the main difference between the mandible and maxilla? +
The mandible is the lower jaw and the only movable bone in the skull. The maxilla is the fixed upper jaw that forms the midface platform. They differ in location, mobility, and which aspects of facial appearance they primarily influence.
Does the maxilla or mandible have a bigger impact on facial attractiveness? +
Neither dominates independently. Attractiveness research consistently points to the relationship between the two bones as the key driver of facial harmony. A well-projected maxilla combined with a defined mandible generally produces more balanced facial aesthetics than optimizing only one.
Can adults change their mandible or maxilla without surgery? +
Significant skeletal changes in adults are very difficult without surgical intervention, since bone sutures fuse after growth is complete. Non-surgical approaches like mewing may influence soft tissue and muscle tone, but evidence for meaningful bone-level change in adults is limited.
What is the gonial angle and why does it matter? +
The gonial angle is the angle formed at the corner of the mandible where the horizontal body meets the vertical ramus. Angles in the range of roughly 115 to 125 degrees are often associated with a sharper, more defined jaw appearance. Very obtuse angles tend to produce a softer, rounder lower face contour.