Good vs Bad Maxilla: What the Difference Looks Like
Learn what separates a good vs bad maxilla, how each affects your facial appearance, and what you can actually do to improve your midface structure.
The maxilla is one of the most consequential bones in your face, yet most people have never heard of it. It forms the upper jaw, the floor of your eye sockets, part of the roof of your mouth, and the base of your nose. In short, it anchors a huge portion of your midface. Whether your maxilla is well-developed or underdeveloped has a visible, measurable impact on how you look.
This guide breaks down exactly what a good vs bad maxilla looks like, what causes the difference, and what options exist for people who want to improve their midface structure.
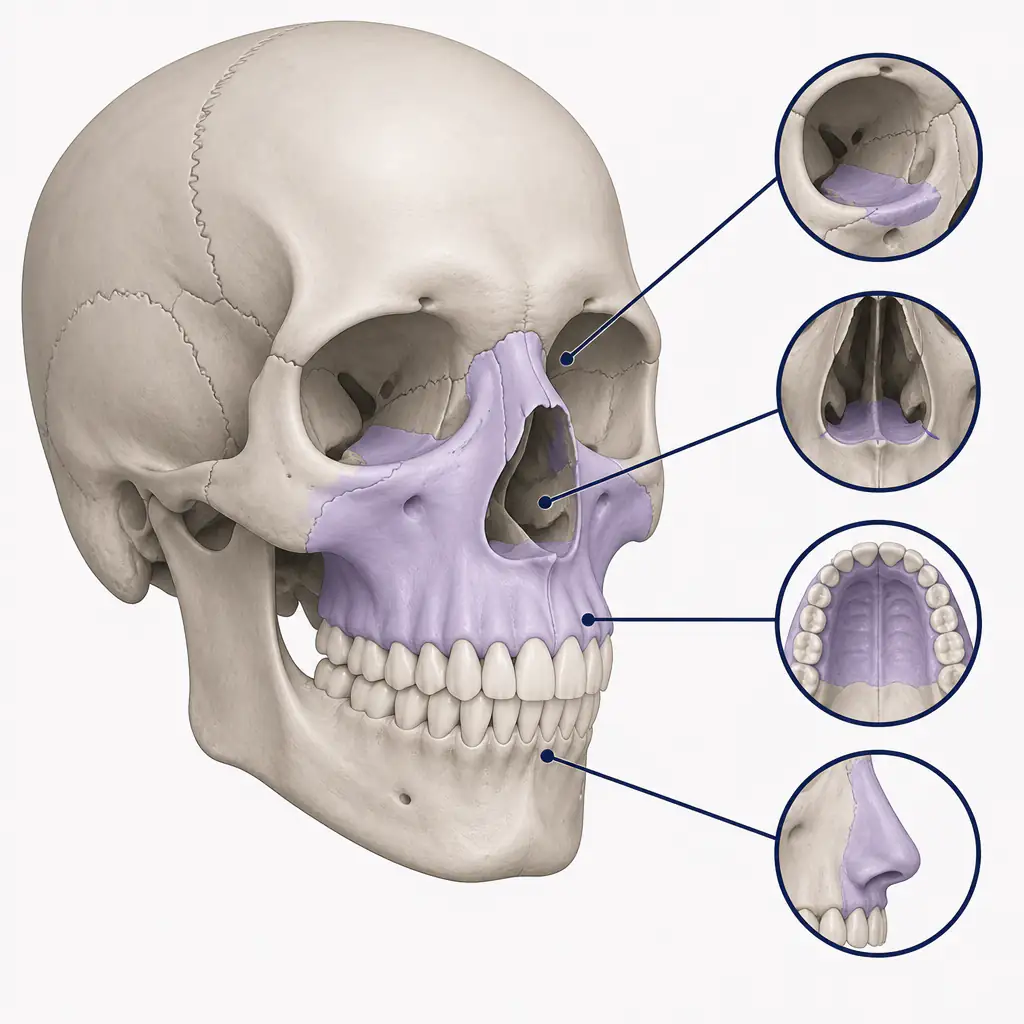
What Is the Maxilla, Exactly?
The maxilla is a paired bone, meaning you have a left and right half that fuse at the midline. Together they form:
- The upper jaw and the sockets for your upper teeth
- The floor of the nasal cavity
- The floor of the orbital sockets (your eye sockets)
- The front portion of the hard palate (roof of your mouth)
Because of how many structures the maxilla supports, its position and size ripple outward to affect your cheekbones, the projection of your nose, the spacing of your eyes, the shape of your lips, and the overall three-dimensional projection of your face. A well-developed maxilla pushes everything forward and upward. A deficient one lets things sink inward and downward.
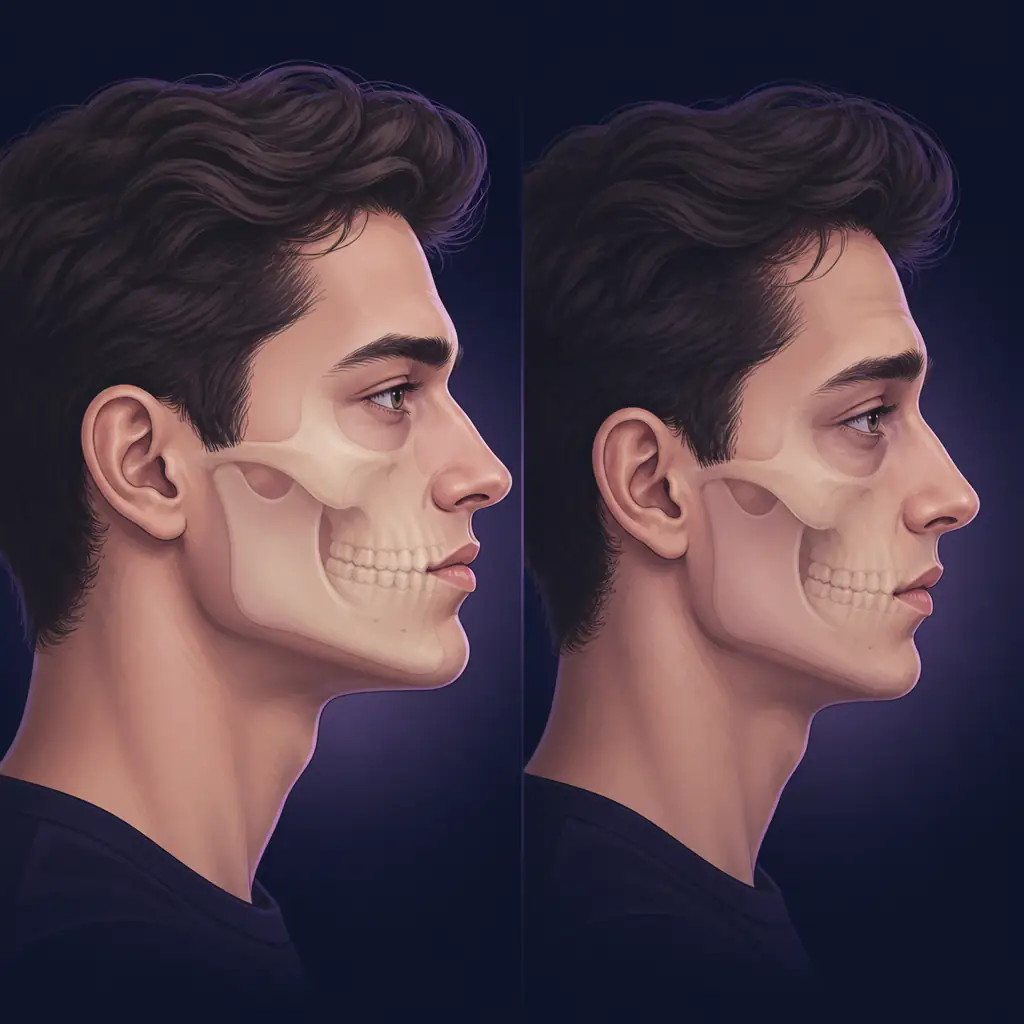
Good Maxilla: What It Looks Like
A good maxilla is characterized primarily by forward projection and vertical sufficiency. Here is what that translates to in visible facial features:
Forward Projection
The midface sits flush with or slightly in front of the rest of the face when viewed from the side. The cheekbones appear prominent. The under-eye area looks full rather than hollow. The nose base is supported, giving the nose a clean, lifted appearance without drooping.
Vertical Sufficiency (Not Too Long, Not Too Short)
The distance from the base of the nose to the upper lip is proportionate. When the mouth is at rest, roughly 2-4 mm of the upper teeth are visible. The upper lip is not hidden behind the lower lip. The face does not look excessively long in the midface region.
Nasal Base Support
Because the maxilla forms the base of the nose, a well-projected maxilla keeps the nasal tip from drooping. The nostrils have a clean, lifted angle.
Strong Eye Support
The orbital floor (bottom of the eye socket) is part of the maxilla. Good maxillary development means the lower eyelid sits at or slightly above the iris, giving what many describe as a positive canthal tilt, and the under-eye area looks supported rather than sunken.
Dental Occlusion
A well-developed maxilla typically allows the upper teeth to sit slightly in front of the lower teeth at rest, known as a Class I occlusion. There is enough room in the dental arch for teeth to align without crowding.
Bad Maxilla: What It Looks Like
Maxillary deficiency, often called midface hypoplasia in clinical settings, produces a recognizable pattern of features that compound one another.
Midface Recession
Viewed from the side, the midface appears to sit behind the chin and forehead. The face looks concave or “dished in” in the middle third. This is one of the clearest signs of a deficient maxilla.
Hollow Under-Eyes
When the orbital floor lacks forward projection, the soft tissue under the eyes loses bony support. The result is the appearance of dark circles, sunken tear troughs, and a tired look regardless of sleep quality.
Flat or Recessed Cheekbones
The cheekbones are partly supported by the upper portion of the maxilla. A deficient maxilla often corresponds with flat or posteriorly positioned cheekbones, reducing the structured look that many associate with an attractive midface.
Elongated or Compressed Midface
Maxillary deficiency can manifest vertically in two directions. Vertical excess makes the midface look long, with too much upper lip length and a gummy smile. Vertical deficiency compresses the midface and can reduce upper lip show entirely.
Dental and Breathing Issues
A narrow or recessed maxilla often corresponds with a high, narrow palate. This can cause dental crowding, an anterior open bite, and in some cases restricted nasal airway because the floor of the nasal cavity is also the roof of the mouth. Mouth breathing is common in people with significant maxillary deficiency and can itself reinforce poor facial development over time.
Lip Posture
Because the upper lip drapes over the front face of the maxilla, a recessed maxilla often results in the upper lip appearing thin, retruded, or unsupported. The lower jaw can appear to protrude in comparison, even when the lower jaw is actually normal in size.
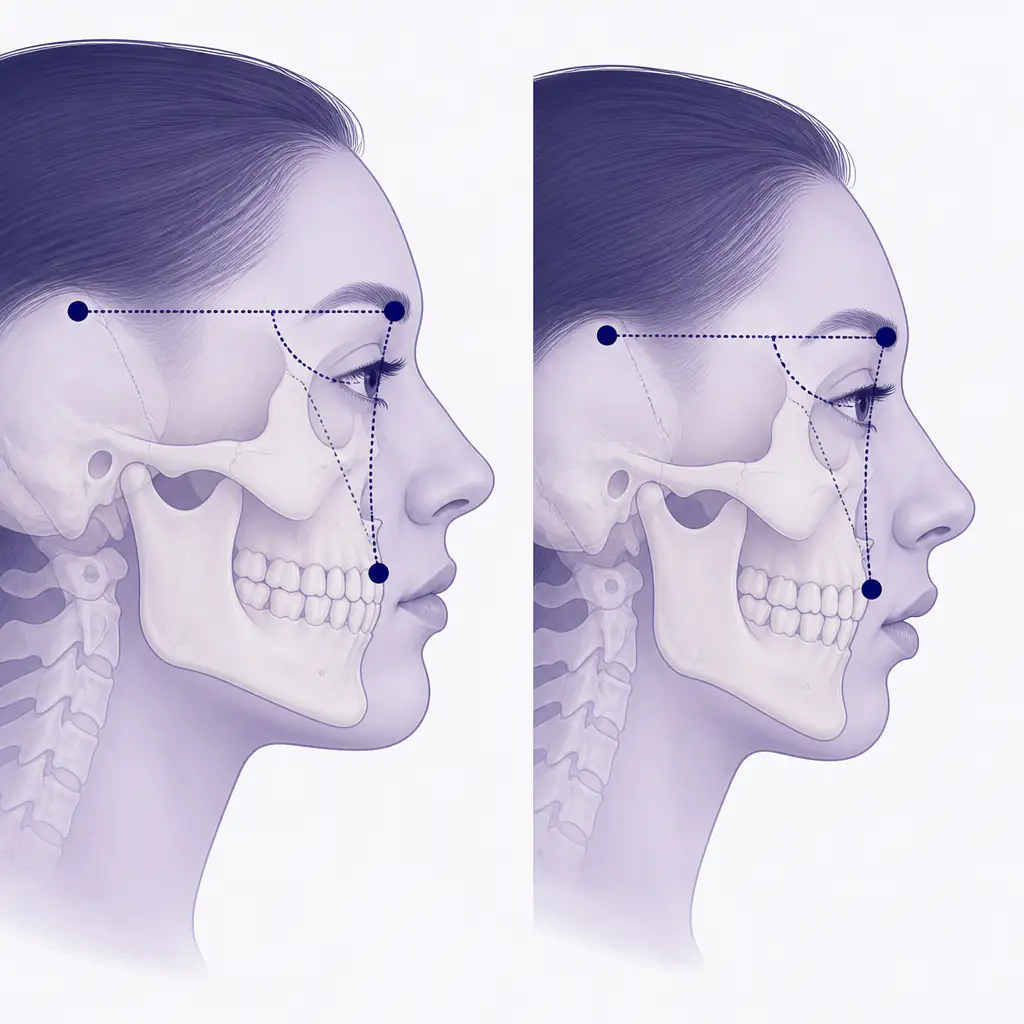
Good vs Bad Maxilla: Side-by-Side Comparison
| Feature | Good Maxilla | Bad Maxilla |
|---|---|---|
| Profile projection | Midface projects forward, flush or ahead of chin | Midface recessed, “dished-in” profile |
| Under-eye area | Full, supported, minimal dark circles | Hollow, sunken tear troughs |
| Cheekbones | Prominent and forward | Flat or recessed |
| Nose appearance | Base supported, tip lifted | Drooping tip, poor nasal base |
| Upper lip | Full, visible at rest, well-supported | Thin, retruded, hidden |
| Dental occlusion | Class I, upper teeth slightly forward | Class III tendency or open bite |
| Upper teeth show | 2-4 mm visible at rest | None visible, or excessive (gummy smile) |
| Palate width | Wide, adequate arch space | Narrow, crowded teeth |
| Eye support | Positive canthal tilt, lower eyelid supported | Negative canthal tilt, scleral show |
| Airway | Open nasal passages | Restricted nasal airway, mouth breathing |
What Causes a Deficient Maxilla?
Maxillary development is determined by a combination of genetics and environmental factors during childhood and adolescence.
Genetic Factors
Inherited bone structure plays a large role. If parents have midface deficiency, children are more likely to as well. Certain ethnic populations also have different average maxillary projection norms.
Mouth Breathing
This is perhaps the most discussed environmental factor. Chronic mouth breathing during childhood disrupts the normal pressure forces that shape palate width and maxillary projection. The tongue rests low instead of pressing against the palate, the cheeks exert inward pressure unopposed, and the result is a narrower, often more vertically oriented maxilla.
Poor Tongue Posture
Related to mouth breathing, incorrect tongue posture (resting on the floor of the mouth rather than the palate) removes the outward pressure that helps widen the dental arch and support maxillary development.
Diet and Chewing Forces
Research suggests that populations eating harder, more fibrous diets tend to develop broader, more robust facial bones. Soft, processed diets in childhood may reduce the mechanical stimulation that drives bone remodeling.
Thumb Sucking and Extended Pacifier Use
Prolonged habits that push the front teeth forward or distort palatal shape can affect maxillary arch form.
Can You Improve Maxillary Development?
The honest answer depends heavily on your age and the severity of any deficiency.
In Children and Adolescents
This is the window where the most impact is possible without surgery. Orthodontic expanders, such as the rapid palatal expander (RPE), can widen the maxillary arch before the mid-palatal suture fuses (typically in the late teens). Myofunctional therapy to correct tongue posture and eliminate mouth breathing can support proper bone development. Early intervention consistently produces better outcomes than waiting.
In Adults
Once skeletal growth is complete, non-surgical options are more limited but not zero.
- MARPE (Miniscrew-Assisted Rapid Palatal Expansion): A more aggressive orthodontic device that, with the support of micro-implants, can expand the adult palate to some degree. It is not effective for everyone and requires assessment by a qualified orthodontist or oral surgeon.
- Mewing (proper tongue posture): Keeping the tongue resting fully against the palate is sometimes called mewing. Research on whether this remodels adult bone is limited, but it costs nothing, improves airway function in some people, and some users report subtle changes over time. Do not expect dramatic skeletal shifts from tongue posture alone as an adult.
- Orthognathic surgery (jaw surgery): For significant maxillary deficiency, surgical advancement of the maxilla via Le Fort I osteotomy is the most reliable correction. This is a major procedure with real recovery time and risks. Talk to a qualified oral and maxillofacial surgeon before considering this option.
- Facial implants: Cheek and sub-orbital implants can restore the appearance of forward projection without moving the bone itself. They do not change the underlying structure but can address the aesthetic concerns. Again, consult a qualified surgeon.
- Soft tissue approaches: Filler in the tear trough and cheek area can temporarily address the hollowness caused by maxillary recession. Results vary and are not permanent.
If you want a clear-eyed assessment of your own midface before exploring any of these options, Aura provides an AI-based analysis of jaw structure, midface projection, and other key features that can give you a useful baseline to work from.
Practical Habits That Support Maxillary Health
While surgical and orthodontic options are the most impactful for significant deficiency, there are low-cost daily habits that may support better facial structure over time, especially for younger people still developing.
- Breathe through your nose. If you are a chronic mouth breather, identify and address the cause: allergies, deviated septum, enlarged adenoids, or simply habit. Nasal breathing is foundational.
- Correct your tongue posture. Rest the entire tongue against the palate with the lips closed and teeth lightly touching or slightly apart. This is the neutral resting position most associated with favorable facial development.
- Chew harder foods. Incorporate foods that require real chewing effort: raw vegetables, tougher proteins, and dense bread. This provides the mechanical stimulation that may support jaw bone density.
- Maintain good head posture. Forward head posture can shift jaw mechanics and soft tissue distribution. Keeping the head balanced over the spine helps.
- Address sleep habits. Sleep apnea and heavy snoring are often linked to airway restriction that worsens with poor maxillary development. A sleep study can clarify whether this is a factor.
For anyone serious about tracking changes or assessing where they currently stand, using Aura to get scored on specific facial features, including jawline and midface balance, can make the process more systematic and less guesswork-driven.
How Professionals Assess the Maxilla
If you are considering orthodontic or surgical intervention, a qualified professional will typically use:
- Lateral cephalometric X-ray: A side-view skull X-ray that allows precise measurement of bone positions relative to standard anatomical landmarks. The angle SNA (Sella, Nasion, A-point) is one common measurement of maxillary forward position.
- CBCT scan (cone beam CT): A three-dimensional scan that gives a full picture of bone structure, airway volume, and dental relationships.
- Clinical examination: Visual assessment of dental occlusion, facial thirds, and soft tissue.
A normal SNA angle is roughly 80-82 degrees. Values significantly below this suggest maxillary retrusion. Values significantly above suggest excess forward projection. These are population averages, not absolutes, and should be interpreted in the context of your full facial structure.
Frequently asked questions
How do I know if I have a bad maxilla? +
Common signs include a recessed or "dished-in" midface profile, hollow under-eyes, flat cheekbones, a thin or retruded upper lip, dental crowding, and a tendency to breathe through the mouth. A lateral cephalometric X-ray assessed by an orthodontist or oral surgeon gives a definitive measurement. You can also get a preliminary sense of your midface projection using AI face analysis tools like Aura.
Can adults improve their maxilla without surgery? +
To a limited degree. MARPE (Miniscrew-Assisted Rapid Palatal Expansion) can widen the adult palate when performed by a specialist. Proper tongue posture and nasal breathing may support subtle soft tissue changes. For significant skeletal deficiency, orthognathic surgery remains the most effective option. Always consult a qualified oral and maxillofacial surgeon before pursuing surgical routes.
Does mewing actually fix a bad maxilla? +
Mewing, or maintaining correct tongue posture against the palate, is a legitimate concept rooted in myofunctional therapy. It is most impactful during childhood and adolescence when bone is still adapting. In adults, the evidence for significant skeletal remodeling from tongue posture alone is limited. It may support airway function and some soft tissue changes, but it is unlikely to correct a meaningful structural deficiency on its own.
What is the difference between maxillary deficiency and a weak chin? +
These are separate but sometimes co-occurring issues. Maxillary deficiency means the upper jaw and midface are underdeveloped or recessed. A weak chin (mandibular retrusion) means the lower jaw sits too far back. Both affect facial profile, but they involve different bones and require different interventions. It is possible to have one without the other, or to have both.