Flat vs Recessed Maxilla: Key Differences Explained
Learn the difference between a flat vs recessed maxilla, how each affects your face, and what you can realistically do about it.
The maxilla is one of the most discussed bones in facial aesthetics, and for good reason. It sits at the structural center of your face, influencing everything from your cheekbone projection to your lip support, eye area, and the way your lower face fits together. Two terms that come up constantly in this space are “flat maxilla” and “recessed maxilla,” and while they are often used interchangeably, they actually describe distinct structural patterns with different visual effects.
Understanding the difference is not just academic. It changes how you assess your own face, what interventions are relevant, and what expectations you should hold. This article breaks down both conditions clearly, compares them directly, and covers what the research says about potential corrections.
What Is the Maxilla and Why Does It Matter?
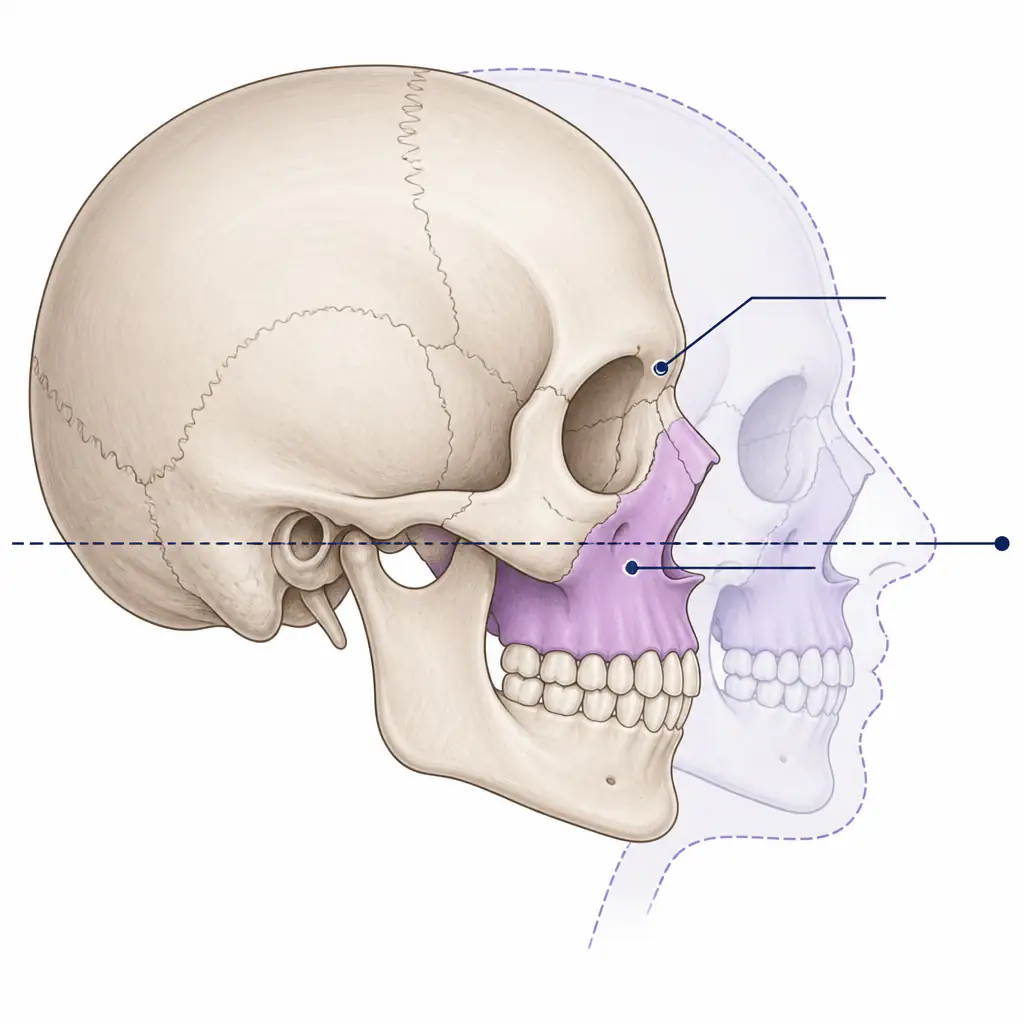
The maxilla is a paired facial bone that forms most of the upper jaw, the floor of the nasal cavity, and a significant portion of the orbital floor (the base of your eye socket). It also holds your upper teeth and contributes directly to midface volume.
Because it sits so centrally, the position and development of the maxilla has cascading effects:
- Lip support: A well-projected maxilla pushes the upper lip forward, creating fullness without filler.
- Cheek appearance: Maxillary projection contributes to the illusion of high cheekbones.
- Under-eye area: The orbital rim support from the maxilla affects how deep-set or hollow your under-eyes appear.
- Lower face: The mandible (lower jaw) follows the maxilla. If the upper jaw is underdeveloped, the lower jaw often compensates awkwardly.
- Airway: Maxillary position affects nasal breathing and oral posture, which in turn affect facial development over time.
When the maxilla develops or sits in a suboptimal position, the effects show up across the entire face, not just locally.
Defining a Flat Maxilla
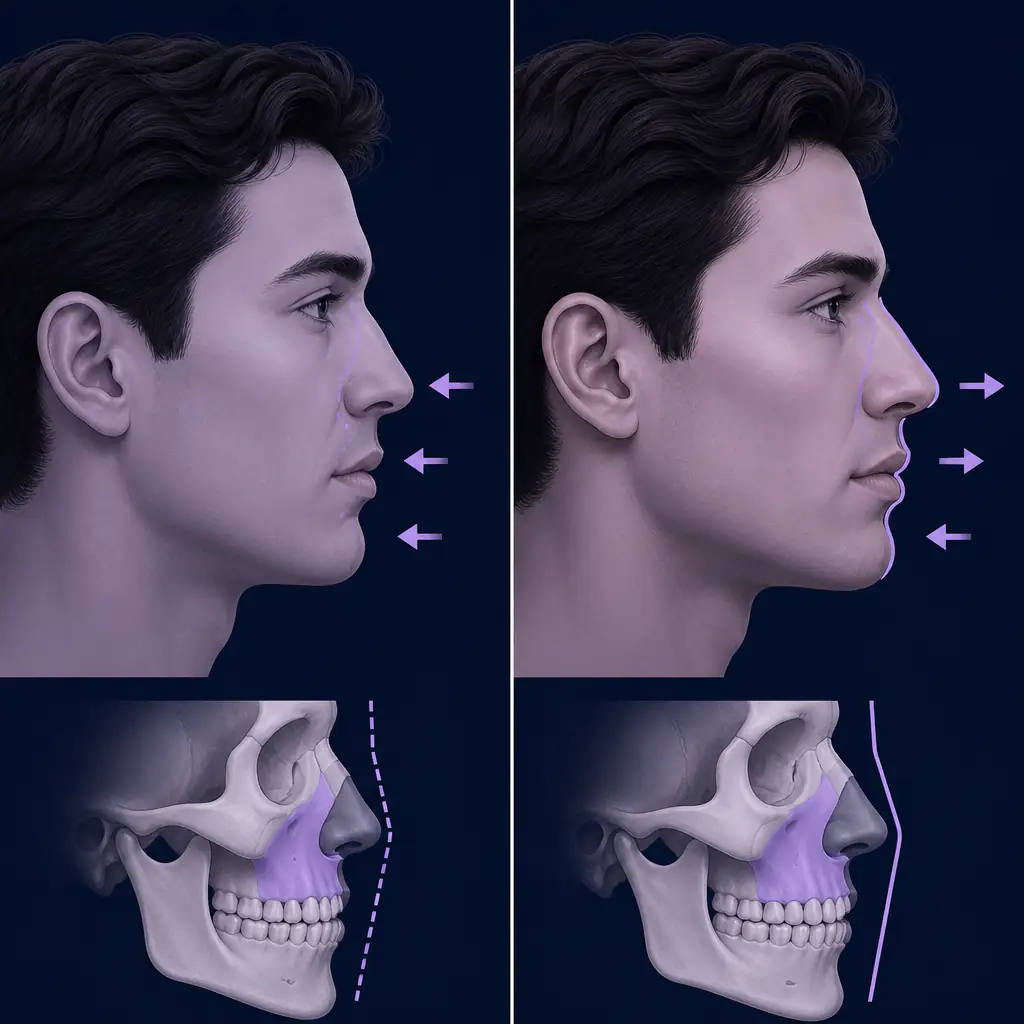
A flat maxilla refers specifically to a lack of forward projection in the midface. The bone is present and structurally intact, but it does not protrude outward sufficiently in the sagittal plane (front-to-back axis). When viewed from the side, a person with a flat maxilla may appear to have a sunken or deflated midface even if the rest of their features are proportionate.
Visual signs of a flat maxilla
- Minimal cheekbone definition when viewed from the front or three-quarter angle
- A relatively flat or underprojected philtrum (the area between the nose and upper lip)
- The upper lip may appear thin or unsupported, even without volume loss
- Nasolabial folds (lines running from the nose to the corners of the mouth) that appear early or are unusually deep
- A generally two-dimensional appearance to the midface
A flat maxilla is often developmental, meaning it results from insufficient forward growth during adolescence. Genetics, mouth breathing, and poor oral posture are all associated with reduced forward maxillary development.
Defining a Recessed Maxilla
A recessed maxilla describes a bone that is positioned too far back relative to the rest of the face and skull. While flatness is about the external surface of the bone, recession is about the three-dimensional position of the entire structure in relation to the cranial base and the Frankfurt horizontal plane (an anatomical reference line running from the top of the ear canal to the bottom of the eye socket).
In simpler terms: a flat maxilla lacks surface projection, while a recessed maxilla is structurally set back.
Visual signs of a recessed maxilla
- A concave facial profile, where the midface appears scooped inward
- The chin and forehead may appear to protrude relative to the midface, even if the chin is not unusually large
- Class III dental occlusion (underbite) is commonly associated, since the upper teeth sit behind the lower teeth
- Deep-set eyes with pronounced orbital rim exposure (the bony ridge under the eye is visible)
- A shorter-looking midface in proportion to the upper and lower thirds
Recession is typically assessed using cephalometric analysis, which involves X-ray measurements of bone angles and distances. An orthodontist or oral and maxillofacial surgeon uses these measurements to determine whether the maxilla itself is recessed or whether adjacent structures are simply more prominent.
Flat vs Recessed Maxilla: A Direct Comparison
Here is a side-by-side breakdown of how these two conditions differ across key dimensions:
| Feature | Flat Maxilla | Recessed Maxilla |
|---|---|---|
| Primary issue | Lack of forward surface projection | Posterior positioning of the entire bone |
| Profile appearance | Midface looks deflated or two-dimensional | Concave midface, face looks “dished” |
| Dental relationship | Usually normal occlusion | Often associated with Class III malocclusion |
| Orbital area | Mild hollowing under eyes | More pronounced orbital rim exposure |
| Chin appearance | May look average | Chin or forehead may appear disproportionate |
| Common cause | Developmental, lifestyle, genetics | Genetics, skeletal growth pattern |
| Assessment method | Visual inspection, 3D imaging | Cephalometric X-ray analysis |
| Soft tissue overlap | Some volume loss may mimic flatness | Bone position is the primary driver |
It is worth noting that the two conditions frequently coexist. A maxilla that is both set back and lacks surface projection will produce a more severe midface deficiency than either condition alone.
How Each Condition Affects Overall Facial Aesthetics
In facial attractiveness research, forward midface projection is consistently associated with higher perceived attractiveness ratings in both male and female faces. The specific mechanisms are debated, but the structural logic is straightforward: forward maxillary development creates natural shadow and light contrast across the cheeks, supports periorbital tissues (the skin around the eyes), and gives the face a three-dimensional quality that reads as healthy bone structure.
For men, a well-projected maxilla contributes to a broader, more angular midface. For women, it supports the high cheekbone aesthetic that is widely considered attractive across multiple cultures.
Conversely, a flat or recessed maxilla tends to flatten the midface, making features look less defined regardless of other positive traits. It can also create the appearance of a longer nose (since the base lacks support) and reduce the visible size of the lips.
If you want an objective read on how your midface currently presents, tools like Aura can provide a structured face analysis including midface assessment, giving you a concrete baseline before you decide how to proceed.
Can You Change Maxillary Position or Projection?
This is where the conversation gets more nuanced, and where honest expectations matter.
Non-surgical approaches
For individuals whose facial skeleton is still developing (generally before the mid-20s), there are legitimate non-surgical options studied in orthodontic literature:
- Mewing and oral posture: Maintaining the tongue on the roof of the mouth with lips sealed and teeth lightly touching may support forward maxillary development during growth phases. Research on this in adults is limited, but some orthodontists note its role in maintaining midface tone.
- Palate expansion: Devices like the Homeoblock or MSE (Maxillary Skeletal Expander) are used orthodontically to widen the palate and, in some studies, to encourage forward displacement of the maxilla. These require a qualified orthodontist.
- Posture and breathing: Nasal breathing versus mouth breathing has documented effects on craniofacial development in children. In adults, correcting mouth breathing may not reverse existing bone position but could support soft tissue appearance.
Surgical options
For adults with established skeletal patterns, significant changes to maxillary position require surgery. The primary procedure is Le Fort I osteotomy, a jaw surgery in which the maxilla is surgically repositioned forward, backward, or vertically. This is a significant procedure performed by oral and maxillofacial surgeons and is typically indicated for functional reasons (bite correction, airway improvement) as well as aesthetic ones.
For surface projection without repositioning the bone, midface implants (specifically zygomaticomalar implants or paranasal implants) can add volume and projection to the flat maxilla region without altering skeletal position.
Soft tissue fillers in the midface can approximate some of the visual effects of better maxillary projection, though results are temporary and carry their own risk profile.
Talk to a qualified professional, such as a board-certified oral and maxillofacial surgeon or orthodontist, before considering any surgical or orthodontic intervention for maxillary positioning.

Practical Steps for Assessing Your Own Maxilla
Before pursuing any change, it helps to have a clear picture of where you actually stand.
- Take a neutral side-profile photo. Use natural lighting and a straight camera angle. Look for whether your midface (the zone from your lower eyelids to your upper lip) projects forward relative to your forehead and chin.
- Check your bite. Do your upper front teeth comfortably sit in front of your lower front teeth when biting down? If your lower teeth sit in front, a recessed maxilla is more likely.
- Assess the under-eye area. Significant orbital rim show (visible bony ridge under the eye) combined with a hollow under-eye area can indicate poor maxillary support.
- Consult a cephalometric analysis. If you suspect genuine skeletal recession rather than just soft tissue flatness, a lateral cephalogram ordered by an orthodontist or oral surgeon is the gold-standard assessment.
- Get a structured face analysis. Aura provides detailed facial scoring and midface assessment, which can help you identify weak points objectively and prioritize your focus areas before committing to any intervention.
The Lifestyle and Habit Angle
Regardless of where your current maxillary development sits, several habits may support the best possible soft-tissue presentation of your midface:
- Maintain a healthy body fat percentage. Excess facial fat can obscure midface definition. Lower body fat generally improves the apparent structure of the cheekbone and midface region.
- Practice nasal breathing. Chronic mouth breathing is associated with downward facial growth and reduced forward projection over time.
- Improve oral posture. Whether or not mewing produces bone changes in adults, proper tongue posture may contribute to better muscle tone in the midface and improved jaw appearance.
- Resistance training. General fitness increases testosterone and growth hormone in ways that may support facial structure tone, though direct effects on bone are modest in adults.
- Sleep quality and hydration. Under-eye hollowing, which worsens the appearance of orbital rim show associated with a recessed maxilla, is significantly influenced by sleep and hydration status.
None of these approaches will reposition an adult maxilla on their own. But they can meaningfully affect how your existing bone structure presents to the world.
Summary
A flat maxilla and a recessed maxilla are related but distinct conditions. Flatness refers to insufficient surface projection, producing a two-dimensional midface appearance. Recession refers to the entire bone sitting too far back relative to the skull, producing a concave profile and often a misaligned bite. Both conditions reduce midface definition and can affect perceived attractiveness.
Understanding which condition applies to you, or whether both do, is the starting point for any rational approach to improvement. Non-surgical options are limited for adults but worth exploring under professional guidance. Surgical options exist and are effective but represent significant interventions that require careful professional evaluation.
Start with an honest assessment of your current facial structure, set realistic expectations, and work systematically from there.
Frequently asked questions
What is the main difference between a flat maxilla and a recessed maxilla? +
A flat maxilla lacks forward surface projection, making the midface look two-dimensional or deflated. A recessed maxilla refers to the entire bone being positioned too far back relative to the skull, which creates a concave facial profile and is often linked to a misaligned bite. The two conditions can occur together but describe different structural issues.
Can a recessed or flat maxilla be fixed without surgery? +
In adults, meaningful changes to maxillary bone position typically require surgical intervention such as a Le Fort I osteotomy. Non-surgical approaches like oral posture habits and palate expansion devices may have some effect during facial development phases but have limited evidence for producing significant bone changes in fully developed adults. Soft tissue fillers can approximate better midface projection temporarily.
How do I know if my maxilla is recessed or just flat? +
A lateral profile photo can reveal whether your midface appears concave or simply flat. Checking your bite is also informative: if your lower teeth sit in front of your upper teeth, skeletal recession is more likely. For a definitive assessment, a cephalometric X-ray analyzed by an orthodontist or oral and maxillofacial surgeon is the most reliable method.
Does mewing help with a flat or recessed maxilla in adults? +
The evidence for mewing producing measurable bone changes in adults is limited. Some researchers suggest it may support soft tissue tone and oral posture habits that influence midface appearance marginally, but it is unlikely to reposition established adult bone structure. Its strongest documented effects relate to facial development during adolescence, not adult correction.