Flat Maxilla: Causes, Effects & How to Fix It
Learn what a flat maxilla is, how to tell if you have one, and what options exist to address a recessed upper jaw for better facial structure.
A flat maxilla is one of the most commonly discussed structural issues in facial aesthetics, yet most people have never heard the term. If you have been told your face looks “pushed in,” if your under-eye area appears hollow, or if your profile lacks definition, your maxilla may be a contributing factor. This guide breaks down what the maxilla is, how to tell if yours is recessed, and what options, both conservative and clinical, are available.
What Is the Maxilla?
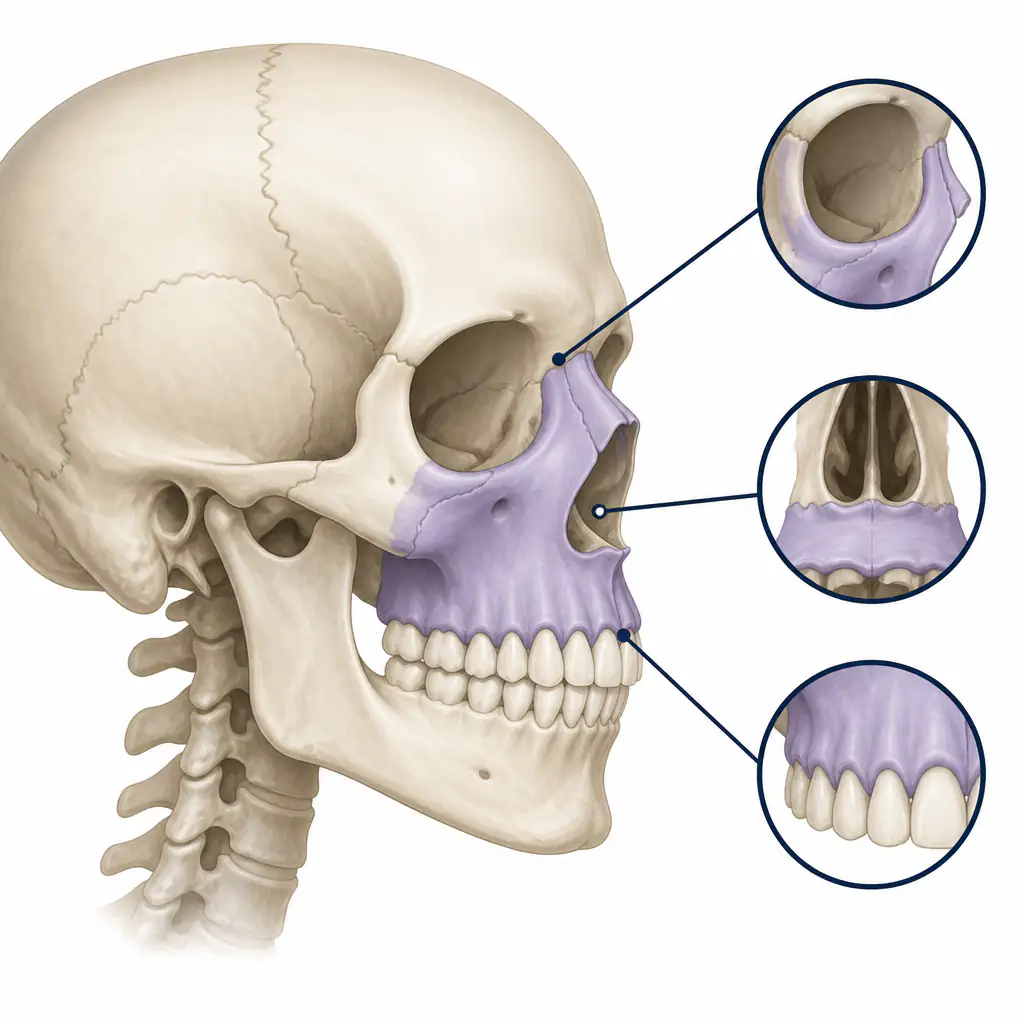
The maxilla is the central bone of the face. It forms the upper jaw, the floor of the eye sockets, the hard palate, and the base of the nose. It is not one isolated structure sitting in the middle of your face; it connects to nearly every other facial bone and anchors your upper teeth.
Because of its central position, the development of the maxilla has a downstream effect on almost everything else. A well-developed maxilla supports the cheekbones, keeps the lower eyelids taut, defines the midface, and holds the upper teeth in a forward position. A flat or recessed maxilla does the opposite.
The upper maxilla (the portion just below the nose and above the upper lip) is particularly visible in profile view. When it lacks forward projection, the whole midface appears to recede, making the nose look larger than it is and the lower face appear to protrude forward by comparison.
Mandible vs Maxilla: Understanding the Difference
The mandible is the lower jaw. The maxilla is the upper jaw. They are distinct bones, and confusion between them is common.
In facial analysis:
- The mandible contributes to the jawline, chin projection, and lower facial width.
- The maxilla contributes to cheek support, midface projection, upper lip support, and the angle of the orbital rim (eye socket).
Some people have a strong mandible but a flat maxilla. This creates a specific look: a defined jawline but a recessed or hollow midface, dark under-eye circles, and a lack of cheekbone prominence. Others have both a recessed maxilla and a weak mandible, resulting in a generally underdeveloped facial profile.
Understanding which bone is the limiting factor matters before exploring any corrective path.
What Does a Flat Maxilla Look Like?
A recessed maxilla produces a recognizable set of visual cues. None of these alone confirms anything, but a cluster of them together is a strong signal:
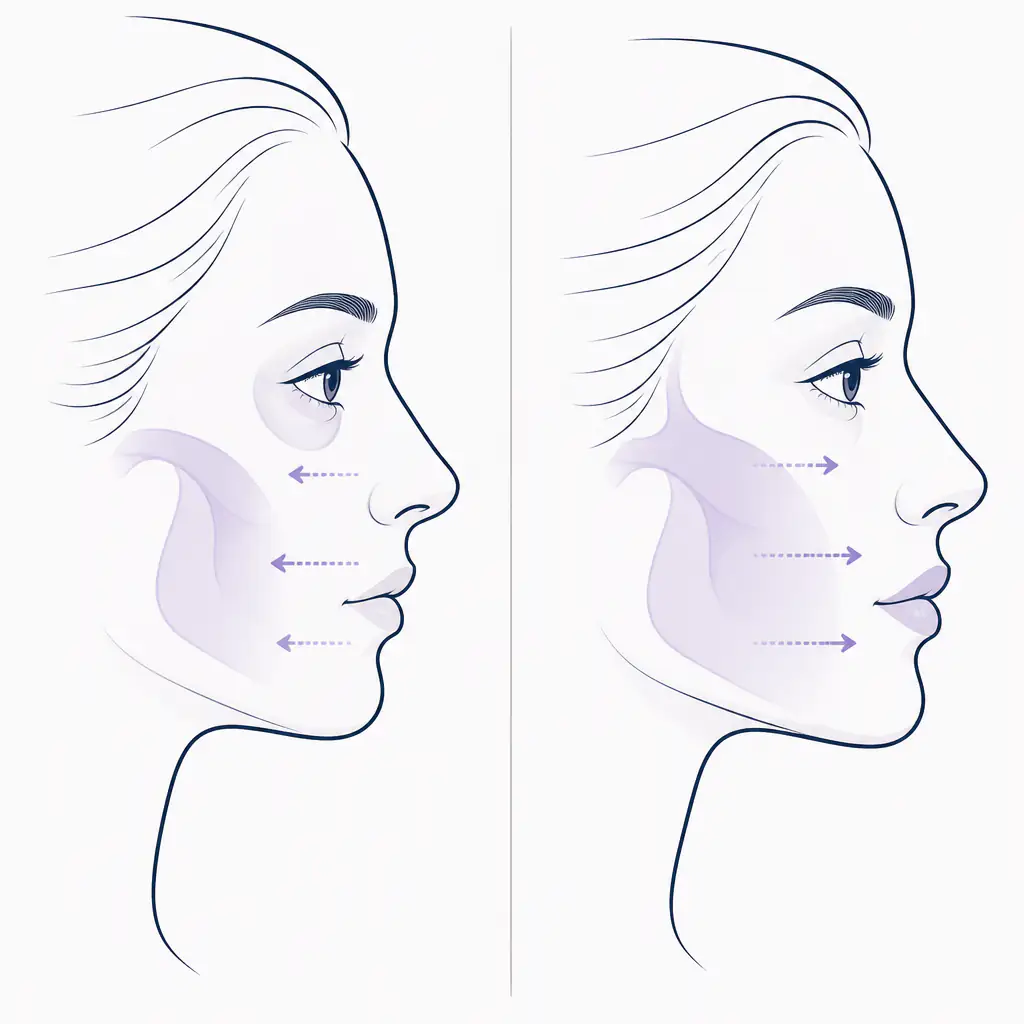
- Hollow or sunken under-eye area (also called a “tear trough” or negative orbital vector)
- Flat or absent cheek projection, particularly below the eye
- A recessed upper lip that appears tucked in rather than supported
- Visible or prominent nose that appears larger than it is in proportion
- Upper maxilla recessed behind the lower lip when viewed from the side
- Increased nasolabial fold depth from lack of midface support
- Gummy smile or visible upper teeth at rest, sometimes associated with vertical maxillary excess (downward growth rather than forward)
A projected maxilla, by contrast, supports the cheeks, keeps the under-eye area full, and creates forward facial projection in profile. A good maxilla is often described in aesthetic terms as one that sits forward relative to the skull base, with the cheekbones and orbital rim in a plane that supports the soft tissue above.
Recessed vs Normal Maxilla: How to Tell If You Have One
Knowing how to tell if you have a recessed maxilla does not require a specialist visit as a first step. These are practical self-assessment methods:
The Profile Test
Take a strict side-on photo in natural lighting. Draw an imaginary vertical line down from your forehead. A well-projected maxilla will have the cheek and upper lip area close to or touching this line. If your midface falls significantly behind the forehead and chin, forward projection may be lacking.
The Orbital Rim Check
Place your finger on your lower eyelid and press gently inward. If your finger sinks back before hitting bone, your orbital rim (part of the maxilla) may be recessed. If bone is immediately behind the lower lid, projection is likely adequate.
Worm’s Eye View Photo
A photo taken slightly below face level looking upward will reveal whether the midface is forward of the lower face. If the lower jaw visually dominates in this angle and the midface disappears, maxillary retrusion may be present.
Professional Cephalometric Analysis
For a definitive answer, a cephalometric X-ray analyzed by an orthodontist or oral and maxillofacial surgeon gives objective measurements. The SNA angle (sella-nasion-A point) measures upper jaw projection relative to the skull base. An SNA below 80 degrees typically indicates a recessed maxilla.
If you want an accessible starting point, Aura provides an AI-based facial analysis that scores midface projection and flags structural patterns like a recessed upper maxilla, which can help you frame the right questions before a clinical consultation.
What Causes a Flat Maxilla?
Maxillary development is influenced by a combination of genetics, breathing patterns during childhood, and oral posture. Key contributing factors include:
- Mouth breathing: Chronic mouth breathing during childhood disrupts the normal forward and lateral growth of the maxilla. The tongue, which should rest on the palate, drops away, removing the internal force that guides outward and forward bone growth.
- Genetics: Skeletal patterns run in families. If one or both parents have midface retrusion, the likelihood increases.
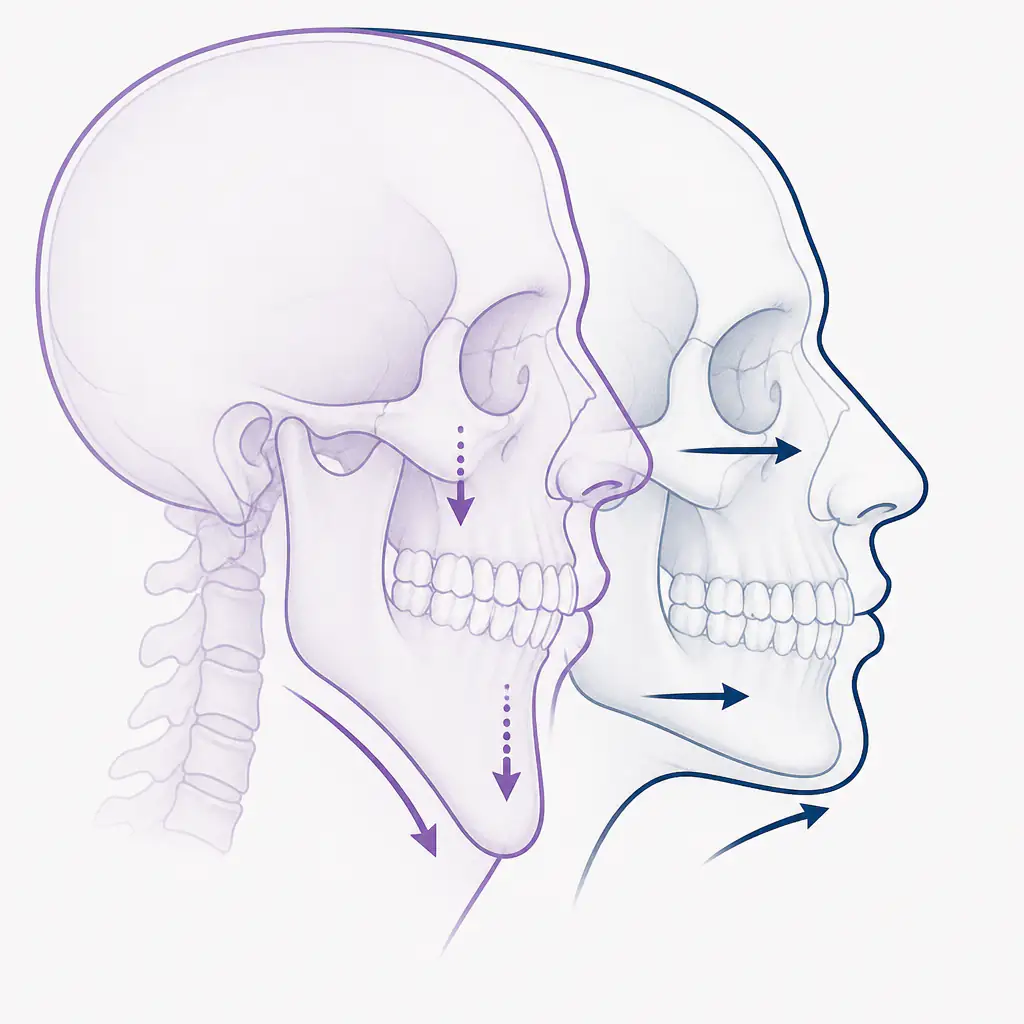
- Downward growth pattern: Some individuals develop a downward growth pattern rather than a forward one. The maxilla descends vertically instead of projecting anteriorly. This often correlates with a long lower facial height, gummy smile, and open bite.
- Early tooth loss or prolonged pacifier use: May affect arch development in younger years.
- Allergies and chronic nasal congestion: These often lead to habitual mouth breathing, which reinforces unfavorable growth patterns.
How to Fix a Recessed Maxilla
Options range from non-invasive habits to significant surgical procedures. The right approach depends on age, severity, and individual goals. Always talk to a qualified professional before considering any clinical intervention.
Mewing and Oral Posture (Conservative)
Mewing refers to maintaining correct oral posture: tongue flat against the palate, lips sealed, breathing through the nose. The claim is that sustained tongue pressure may guide forward and lateral maxillary growth over time, particularly in younger individuals whose sutures have not fully fused.
Research on adult bone remodeling through oral posture alone is limited. Some practitioners and researchers suggest that sutures remain at least partially responsive into early adulthood, while others are skeptical. For younger users, the habit carries low risk and may produce modest structural benefit.
Palatal Expansion
For individuals still in growth phases, palatal expanders can widen the maxillary arch. Rapid palatal expansion (RPE) is a well-established orthodontic tool for adolescents. In adults, MARPE (miniscrew-assisted rapid palatal expansion) can expand the palate using skeletal anchorage, bypassing the fused midpalatal suture. Some research suggests this also produces modest forward movement in addition to lateral expansion.
Orthodontic Camouflage
In cases where the skeletal discrepancy is mild, orthodontics can reposition teeth to improve the appearance of lip support and smile aesthetics without changing the underlying bone. This does not address the structural issue but can meaningfully improve aesthetics.
Orthognathic Surgery (Le Fort I Osteotomy)
For significant maxillary retrusion, the most effective solution is Le Fort I osteotomy, a surgical procedure that detaches the maxilla from the skull base and moves it forward, upward, or downward depending on the treatment plan. This is typically done in combination with mandibular surgery for comprehensive correction.
Results are predictable and can substantially alter facial aesthetics and function (bite, airway, lip support). Recovery is significant, and cost is high. This is not a casual decision. Consult an oral and maxillofacial surgeon or a craniofacial specialist with extensive experience in orthognathic cases.
Midface Implants
Silicone implants placed over the submalar or malar region can improve the appearance of midface projection without moving bone. They address the aesthetic issue rather than the skeletal one, but are a relevant option for adults who do not want or qualify for orthognathic surgery.
How to Get Forward Growth: Practical Habits Worth Building
Whether or not you pursue any clinical route, certain foundational habits support the best possible facial development and soft-tissue appearance:
- Fix your breathing: Address any nasal obstruction. Mouth tape at night is a simple experiment; see an ENT if you have structural causes like a deviated septum.
- Maintain oral posture: Tongue on palate, teeth lightly together, lips closed.
- Chew harder foods: Some evidence suggests that chewing tougher foods maintains bone density and may provide low-level mechanical stimulus to the midface.
- Reduce body fat: Lower body fat increases midface definition and makes existing bone structure more visible. A flat maxilla is harder to detect at higher body fat percentages and more obvious at lower ones.
- Sleep position: Some practitioners suggest back sleeping or avoiding pressure on the face during sleep, though evidence here is mostly anecdotal.
- Posture: Forward head posture affects how the jaw develops and how the face is perceived. Addressing neck and thoracic posture has downstream effects on facial presentation.
For a structured way to track where you stand and identify your biggest structural priorities, Aura offers a detailed breakdown of facial features including jawline, under-eye area, and midface projection, giving you a clear baseline to work from.
Bad Maxilla vs Good Maxilla: A Quick Comparison
| Feature | Recessed / Bad Maxilla | Projected / Good Maxilla |
|---|---|---|
| Under-eye area | Hollow, dark circles | Full, supported lower lid |
| Cheek projection | Flat or absent | Forward, defined |
| Upper lip support | Thin, recessed | Full, forward |
| Profile | Concave midface | Straight or convex midface |
| Orbital vector | Negative (eye ahead of cheek) | Neutral to positive |
| Nose appearance | Appears large, droopy | Proportionate |
| Lower face | Appears to protrude | Balanced with midface |
None of these individual features is diagnostic on its own. Facial aesthetics are multidimensional, and multiple bones contribute to any given feature. The table above is a pattern guide, not a checklist for self-diagnosis.
Key Takeaways
- The maxilla is the central bone of the face and has wide-reaching effects on facial aesthetics and function.
- A flat or recessed maxilla produces hollow under-eyes, flat cheeks, poor lip support, and a receded midface in profile.
- Causes include genetics, mouth breathing, and downward rather than forward growth patterns.
- Self-assessment is possible through profile photos and the orbital rim check, but cephalometric imaging gives objective data.
- Options range from oral posture habits and expansion devices to surgery, depending on age and severity.
- Talk to a qualified professional before pursuing any clinical or surgical intervention.
Frequently asked questions
What is a flat maxilla? +
A flat maxilla is a maxilla that lacks forward projection relative to the rest of the skull. Instead of sitting prominently in the midface, it is recessed, which creates a hollow under-eye area, flat cheeks, reduced upper lip support, and a concave appearance in profile.
How do I know if my upper maxilla is recessed? +
Common signs include a hollow tear-trough area under the eyes, flat cheeks, a receded upper lip in side profile, and a negative orbital vector where the eye appears to protrude past the cheek. A cephalometric X-ray with an SNA angle below 80 degrees is the most objective indicator, and an orthodontist or oral surgeon can assess this properly.
Can mewing fix a flat maxilla in adults? +
Mewing (correct oral posture with the tongue on the palate) may provide modest benefits in younger individuals whose facial sutures are still active. In adults, the evidence for significant bone remodeling through oral posture alone is limited. It is a low-risk habit worth maintaining, but adults with significant maxillary retrusion typically need orthodontic or surgical intervention for meaningful structural change.
What is the difference between the maxilla and the mandible? +
The maxilla is the upper jaw, forming the midface, upper teeth, cheek base, and orbital floor. The mandible is the lower jaw, forming the chin and lower facial frame. They work together in bite function, but their aesthetic contributions are distinct. A recessed maxilla affects the midface and under-eye area, while a weak mandible mainly affects the chin and lower jaw definition.